
Atypical earache can be referred pain from moderate to severe damage jaw joint (TMD)
Repetitive trips to PCP or ENT for earache w/o infection or inflammation or slight inflammation w/o benefit from antibiotic, you have referred pain from TMD.
Atypical Symptoms:
Secondary hints:
Anatomical hints:
ENT difficulty w/ Atypical Earache?
1) Little time was spent in ENT school on jaw joint 2) ENT assumes dentistry covers TMD 3) Dental school left TMD out dental training 3) Cross over pathologies are poorly manged in all fields 4) Insurance doesn't cover interdisplicinary communication 5) Orofacial Pain Specialist referrals are difficult cross dental medical fields 6) Patients looking for quick fix do not honor/trust referral 7) Patient have trouble understanding referred pain
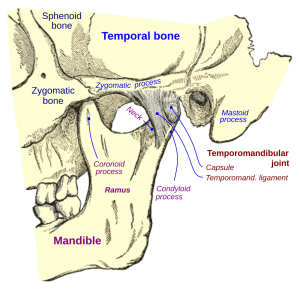
Moderate to severe damage in jaw joint referring into ear:
Hints moderate/severe jaw joint damage:
Tinnitus rarely associated w/ TMD
Disc displacement was found to be present in ipsilateral joint in all 53 patients w/ unilateral tinnitus. (Ren &Isberg. J. CranioPrac 1995 13:75)
TINNITUS
Atypical earache can be referred pain from moderate to severe damage jaw joint (TMD)
Repetitive trips to PCP or ENT for earache w/o infection or inflammation or slight inflammation w/o benefit from antibiotic, you have referred pain from TMD.
Atypical Symptoms:
Secondary hints:
Anatomical hints:
ENT difficulty w/ Atypical Earache?
1) Little time was spent in ENT school on jaw joint 2) ENT assumes dentistry covers TMD 3) Dental school left TMD out dental training 3) Cross over pathologies are poorly manged in all fields 4) Insurance doesn't cover interdisplicinary communication 5) Orofacial Pain Specialist referrals are difficult cross dental medical fields 6) Patients looking for quick fix do not honor/trust referral 7) Patient have trouble understanding referred pain
Moderate to severe damage in jaw joint referring into ear:
Hints moderate/severe jaw joint damage:
Tinnitus rarely associated w/ TMD
Disc displacement was found to be present in ipsilateral joint in all 53 patients w/ unilateral tinnitus. (Ren &Isberg. J. CranioPrac 1995 13:75)
TINNITUS

1) Neck pain: is associated with muscle bracing, posturing, reciprocal
contraction jaw system
…